Skip to content
Did you know there is an actual World Periodic Paralysis Day? It's March 23rd. Click here for more details!
Home
Emergency Care
Expand
Anesthesia
Expand
Anesthesia Quick Reference Guides
Anesthesia, Peri-op Care Literature
Emergency Treatment
Expand
Hypokalemic PP
HyperKPP & PMC
Andersen-Tawil Syndrome
Thyrotoxic (TPP)
About Us
Expand
Mission and History
Board of Directors
Contact Us
Donations
Online Library
Expand
Patient’s Library
D. Greant Library
Additional Resources
Expand
What is Periodic Paralysis
PPSN Doctors List
Expand
Doctors within the USA
Doctors outside the USA
Assistance Organizations
Search for:
Search
Toggle Menu
Scientific
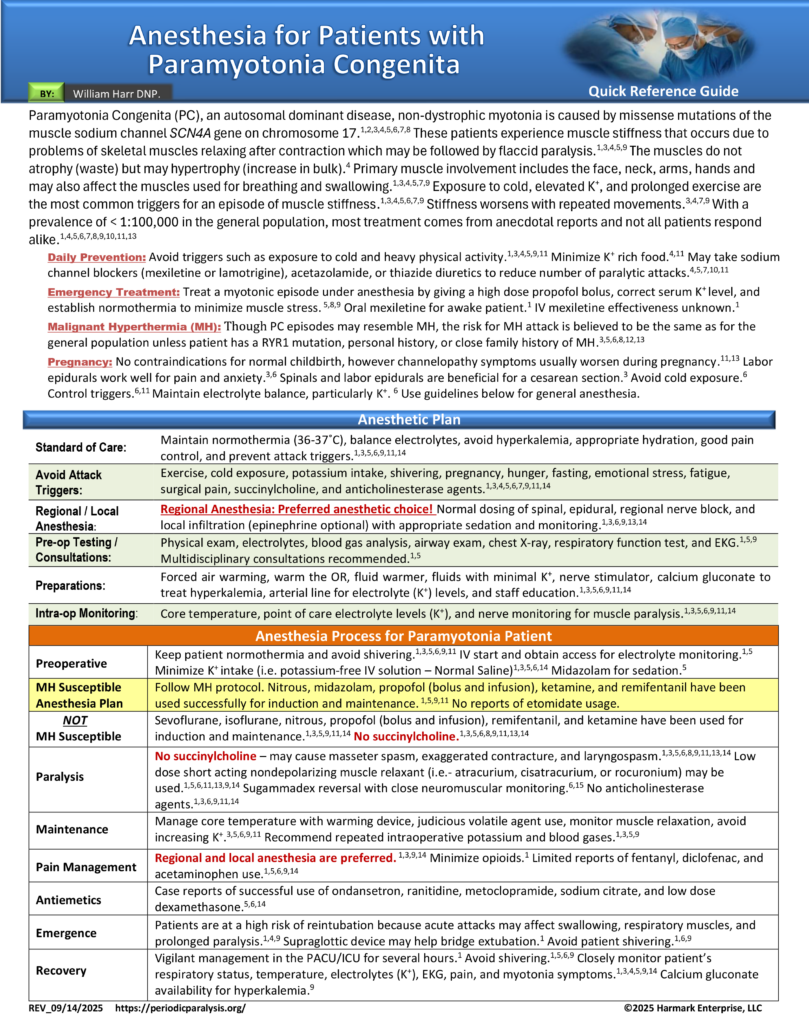
Anesthesia for the Adult Patient with Paramyotonia Congenita
By
William Harr DNP, CRNA
March 1, 2026
March 4, 2026
Click here to download this as a Quick Reference Guide
Post navigation
Previous
Previous
Anesthesia for the Adult Patient with Myotonia Congenita
Home
Emergency Care
Toggle child menu
Expand
Anesthesia
Toggle child menu
Expand
Anesthesia Quick Reference Guides
Anesthesia, Peri-op Care Literature
Emergency Treatment
Toggle child menu
Expand
Hypokalemic PP
HyperKPP & PMC
Andersen-Tawil Syndrome
Thyrotoxic (TPP)
About Us
Toggle child menu
Expand
Mission and History
Board of Directors
Contact Us
Donations
Online Library
Toggle child menu
Expand
Patient’s Library
D. Greant Library
Additional Resources
Toggle child menu
Expand
What is Periodic Paralysis
PPSN Doctors List
Toggle child menu
Expand
Doctors within the USA
Doctors outside the USA
Assistance Organizations
Search
Search
Toggle Menu Close
Search for:
Search