
Using the Transtubular Potassium Concentration Gradient to Determine the Origin of Hypokalemic Paralysis
Many patients with hypokalemic paralysis live in diagnostic limbo for years without appropriate testing and therapy. Since time is muscle in the channelopathies, patients need speedy diagnosis and treatment. Repeated studies have shown that the transtubular potassium concentration gradient (TTKG), easily performed in the ER during an attack, can be used to distinguish between hypokalemia caused by renal (urinary) losses and hypokalemia caused by the intracellular shift of serum potassium into skeletal muscle, as in channelopathy HKPP.
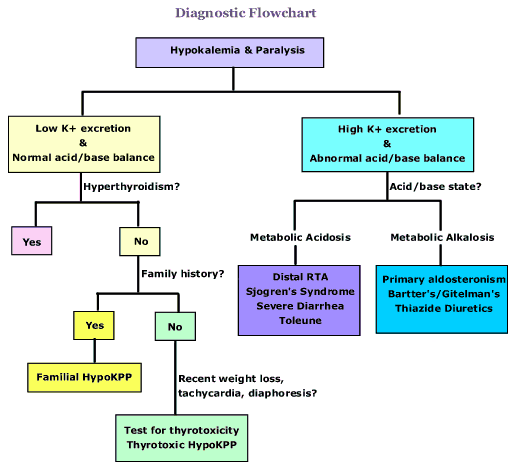
The principle behind the test is that when faced with a low serum K+ level, the kidneys should excrete as little K+ as possible, unless the kidneys are the cause of the hypokalemia. A urinary K+ concentration greater than 20 mmol/L during hypokalemia indicates urinary loss of K+, i.e. hypokalemia of renal origin.
Clues which might indicate hypokalemia associated with intracellular shift are: weakness/paralysis which developed over a short time span (i.e. an hour or less) or during sleep, a low rate of K+ excretion, the absence of a metabolic acid base disorder, large intake of carbohydrate within past 48 hours, life crisis or stress, or signs of hyperthyroidism.
For example: A 13 year-old boy with familial hypokalemic periodic paralysis was observed during a paralytic attack and recovery. On the day of the attack the boy awoke at 5:00 am with complete paralysis. Because he vomited and could not take oral potassium he was admitted to the hospital at 11:00 am for observation and treatment with IV K+. Laboratory tests were done beginning at 11:00 am and for the next 22 hours, until 9:00 am the following day, when he was fully recovered.
SK+ = serum potassium, Total UK+ex = total urine potassium excreted. Urine was collected at 14:00 after 15 hours without urination.
Time________ SK+ ___________Total UK+ ex
11:00 _____ 2.3 mmol/l______0_____
14:00 _____ 3.3 mmol/l _____ 5 mmol
17:00 _____ 4.6 mmol/l ______8 mmol
22:00 _____4.6 mmol/l _______10 mmol
9:00 ______4.7 mmol/l ______ 25 mmol
The normal renal response when hypokalemia is due to non-renal causes is a TTKG less than 2, where a TTKG greater than 5 is indicative of increased secretion of K+ in the cortical collecting ducts. Thus a transtubular potassium concentration gradient (TTKG) of greater than 3.0 indicates hypokalemia of renal origin, while a value below 2.0 indicates intracellular shift of K+, as found in ion channelopathy hypokalemic periodic paralysis.
The transtubular K+ concentration ([K+]) gradient (TTKG) is calculated using the following formula: TTKG = [K+]urine/(urine/plasma)/osmol/[K+]plasma History
1. Eliminate dietary inadequacy, diuretic, thyroid hormone or caffeine abuse, herbal usage (i.e. licorice root) or “body-building” supplements as potential causes of hypokalemia.
2. Recent history of ?: a) Unusual intensity of exercise; b) high carbohydrate intake (inc. alcohol) ; c) stress or life crisis; d) chilling; or e) combination of these factors. Signs consistent with hyperthyroidism or excess of beta-adrenergic activity; recent weight loss, diaphoresis, tachycardia, systolic hypertension, and wide pulse pressure.
3. Has patient experienced exercise intolerance, episodes of weakness or paralysis in past, especially on awakening? (Patients sometimes do not recognize exercise intolerance or paralysis on awakening as abnormal.)
4. Family history: Take a detailed family history; Ask about family members, including cousins, aunts, uncles, grandparents with similar symptoms or unexplained weakness, exercise intolerance, late life development of myopathy in legs? Sometimes attacks are called “spells”, and were believed to be, or were diagnosed as “polio” or a “stroke” which was miraculously “cured” in hours by prayer or an herbal remedy.
References:
1. Alazami M, Lin SH, Cheng CJ, Davids MR, Halperin ML. Unusual causes of hypokalaemia and paralysis. QJM. 2006 Mar;99(3):181-92. Epub 2006 Feb 9. PMID: 16469765
2. Ethier JH, Kamel KS, Magner PO, Lemann J Jr, Halperin ML. The transtubular potassium concentration in patients with hypokalemia and hyperkalemia. Am J Kidney Dis. 1990 Apr;15(4):309-15. PMID: 2321642
3. Joo KW, Chang SH, Lee JG, Na KY, Kim YS, Ahn C, Han JS, Kim S, Lee JS. Transtubular potassium concentration gradient (TTKG) and urine ammonium in differential diagnosis of hypokalemia. J Nephrol. 2000 Mar/Apr;13(2):120-5. PMID: 10858974
4. Lin SH, Lin YF, Halperin ML. Hypokalaemia and paralysis. QJMed 2001 Mar;94(3):133-9. PMID: 11259688
5. Lin SH, Chiu JS, Hsu CW, Chau T. A simple and rapid approach to hypokalemic paralysis. Am J Emerg Med. 2003 Oct;21(6):487-91. PMID: 14574658
6. Lin SH, Davids MR, Halperin ML. Hypokalaemia and paralysis. QJM. 2003 Feb;96(2):161-9. PMID: 12589014
7. Lin SH, Cheema-Dhadli S, Gowrishankar M, Marliss EB, Kamel KS, Halperin ML. Control of excretion of potassium: lessons from studies during prolonged total fasting in human subjects. Am J Physiol Renal Physiol 273: F796-F800, 1997; PMID: 9374844
8. Links TP; Muscle Fiber Conduction Velocity and Serum Muscle Enzymes in a Patient With an Attack of HypoKalemic Periodic Paralysis, Familial Hypokalemic Periodic Paralysis; ISBN 90-9005053-1, Chap 4.4 pp 113 – 122
9. Shih-Hua Lin, Sung-Sen Yang, Tom Chau. A Practical Approach to Genetic Hypokalemia. Electrolytes Blood Press 8:38-50, 2010; PMID: 21468196
Using the Transtubular Potassium Concentration Gradient to Determine the Origin of Hypokalemic Paralysis
Many patients with hypokalemic paralysis live in diagnostic limbo for years without appropriate testing and therapy. Since time is muscle in the channelopathies, patients need speedy diagnosis and treatment. Repeated studies have shown that the transtubular potassium concentration gradient (TTKG), easily performed in the ER during an attack, can be used to distinguish between hypokalemia caused by renal (urinary) losses and hypokalemia caused by the intracellular shift of serum potassium into skeletal muscle, as in channelopathy HKPP.
The principle behind the test is that when faced with a low serum K+ level, the kidneys should excrete as little K+ as possible, unless the kidneys are the cause of the hypokalemia. A urinary K+ concentration greater than 20 mmol/L during hypokalemia indicates urinary loss of K+, i.e. hypokalemia of renal origin.
Clues which might indicate hypokalemia associated with intracellular shift are: weakness/paralysis which developed over a short time span (i.e. an hour or less) or during sleep, a low rate of K+ excretion, the absence of a metabolic acid base disorder, large intake of carbohydrate within past 48 hours, life crisis or stress, or signs of hyperthyroidism.
For example: A 13 year-old boy with familial hypokalemic periodic paralysis was observed during a paralytic attack and recovery. On the day of the attack the boy awoke at 5:00 am with complete paralysis. Because he vomited and could not take oral potassium he was admitted to the hospital at 11:00 am for observation and treatment with IV K+. Laboratory tests were done beginning at 11:00 am and for the next 22 hours, until 9:00 am the following day, when he was fully recovered.
SK+ = serum potassium, Total UK+ex = total urine potassium excreted. Urine was collected at 14:00 after 15 hours without urination.
Time________ SK+ ___________Total UK+ ex
11:00 _____ 2.3 mmol/l______0_____
14:00 _____ 3.3 mmol/l _____ 5 mmol
17:00 _____ 4.6 mmol/l ______8 mmol
22:00 _____4.6 mmol/l _______10 mmol
9:00 ______4.7 mmol/l ______ 25 mmol
The normal renal response when hypokalemia is due to non-renal causes is a TTKG less than 2, where a TTKG greater than 5 is indicative of increased secretion of K+ in the cortical collecting ducts. Thus a transtubular potassium concentration gradient (TTKG) of greater than 3.0 indicates hypokalemia of renal origin, while a value below 2.0 indicates intracellular shift of K+, as found in ion channelopathy hypokalemic periodic paralysis.
The transtubular K+ concentration ([K+]) gradient (TTKG) is calculated using the following formula: TTKG = [K+]urine/(urine/plasma)/osmol/[K+]plasma History
1. Eliminate dietary inadequacy, diuretic, thyroid hormone or caffeine abuse, herbal usage (i.e. licorice root) or “body-building” supplements as potential causes of hypokalemia.
2. Recent history of ?: a) Unusual intensity of exercise; b) high carbohydrate intake (inc. alcohol) ; c) stress or life crisis; d) chilling; or e) combination of these factors. Signs consistent with hyperthyroidism or excess of beta-adrenergic activity; recent weight loss, diaphoresis, tachycardia, systolic hypertension, and wide pulse pressure.
3. Has patient experienced exercise intolerance, episodes of weakness or paralysis in past, especially on awakening? (Patients sometimes do not recognize exercise intolerance or paralysis on awakening as abnormal.)
4. Family history: Take a detailed family history; Ask about family members, including cousins, aunts, uncles, grandparents with similar symptoms or unexplained weakness, exercise intolerance, late life development of myopathy in legs? Sometimes attacks are called “spells”, and were believed to be, or were diagnosed as “polio” or a “stroke” which was miraculously “cured” in hours by prayer or an herbal remedy.
References:
1. Alazami M, Lin SH, Cheng CJ, Davids MR, Halperin ML. Unusual causes of hypokalaemia and paralysis. QJM. 2006 Mar;99(3):181-92. Epub 2006 Feb 9. PMID: 16469765
2. Ethier JH, Kamel KS, Magner PO, Lemann J Jr, Halperin ML. The transtubular potassium concentration in patients with hypokalemia and hyperkalemia. Am J Kidney Dis. 1990 Apr;15(4):309-15. PMID: 2321642
3. Joo KW, Chang SH, Lee JG, Na KY, Kim YS, Ahn C, Han JS, Kim S, Lee JS. Transtubular potassium concentration gradient (TTKG) and urine ammonium in differential diagnosis of hypokalemia. J Nephrol. 2000 Mar/Apr;13(2):120-5. PMID: 10858974
4. Lin SH, Lin YF, Halperin ML. Hypokalaemia and paralysis. QJMed 2001 Mar;94(3):133-9. PMID: 11259688
5. Lin SH, Chiu JS, Hsu CW, Chau T. A simple and rapid approach to hypokalemic paralysis. Am J Emerg Med. 2003 Oct;21(6):487-91. PMID: 14574658
6. Lin SH, Davids MR, Halperin ML. Hypokalaemia and paralysis. QJM. 2003 Feb;96(2):161-9. PMID: 12589014
7. Lin SH, Cheema-Dhadli S, Gowrishankar M, Marliss EB, Kamel KS, Halperin ML. Control of excretion of potassium: lessons from studies during prolonged total fasting in human subjects. Am J Physiol Renal Physiol 273: F796-F800, 1997; PMID: 9374844
8. Links TP; Muscle Fiber Conduction Velocity and Serum Muscle Enzymes in a Patient With an Attack of HypoKalemic Periodic Paralysis, Familial Hypokalemic Periodic Paralysis; ISBN 90-9005053-1, Chap 4.4 pp 113 – 122
9. Shih-Hua Lin, Sung-Sen Yang, Tom Chau. A Practical Approach to Genetic Hypokalemia. Electrolytes Blood Press 8:38-50, 2010; PMID: 21468196