
The periodic paralyses are a group of rare inherited disorders that cause temporary episodes of muscle weakness or paralysis. Periodic Paralysis is found in all races and genders. Some patients have their first attack within minutes of birth, but a few don’t have symptoms until they are in their 60’s or 70’s. Attacks may last only a few moments or go on for days, depending on the type of periodic paralysis the person has. Some forms of periodic paralysis include muscle stiffness as part of the attacks. Some forms include permanent muscle weakness which develops over a period of many years. Some older patients have both paralytic episodes and long-lasting episodes of fatigue and weakness called Abortive Attacks. Some patients have no recognizable attacks of weakness but develop permanent muscle weakness that begins in their 40s or 50s and grows disabling over time.
How do you get periodic paralysis?
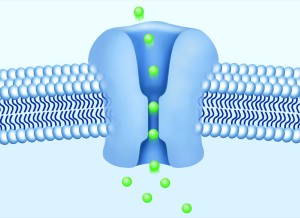
Periodic paralysis is caused by mutations (changes) in the genes that control the function of certain ion channels in the muscle membrane. Ion channels are openings that pierce the muscle membrane and act as gates for the movement of ions of sodium and potassium in and out of the cell. Most cases of periodic paralysis are inherited, but a family history may not be obvious. Only one parent need carry the mutated gene, and that parent may not have any symptoms.
About half of the females and a few men who carry the gene mutation have no symptoms, or have such mild symptoms that they are never diagnosed with periodic paralysis. These people can still pass the gene on to their children. Each child of an affected parent has a 50% chance of inheriting the gene mutation. Unless the parent’s gene mutation has been identified there is no prenatal test available and it is impossible to predict whether a child will inherit the gene. It is also impossible to predict to what degree a child who inherits the mutation will be affected. Even identical twins can be affected to different degrees.
What determines which kind of periodic paralysis I have?
The ion channel which is affected determines the type of periodic paralysis. As of December 2021 approximately 70 different mutations have been identified, affecting sodium, calcium, or potassium channels. However, DNA testing still cannot be relied on entirely for diagnosis. At least 20% of clinically diagnosed patients have mutations that have not yet been identified. A negative DNA test does not rule out a diagnosis of periodic paralysis.
How does a gene mutation cause episodic paralysis?
The movement of sodium and potassium ions from one side of the muscle membrane to the other creates an electrical current. For the muscles to work properly the sodium and potassium ions must be kept in the correct ratio both inside and outside the cell. In periodic paralysis the ion channels fail to regulate the flow of ions properly when potassium levels in the blood fluctuate. The ratio of sodium and potassium inside and outside the cell become unbalanced. The muscle responds less when asked to move, which is felt as weakness. If the imbalance becomes pronounced the muscle quits responding at all, i.e. becomes paralysed.
How many types of periodic paralysis are there?
The Periodic Paralyses include Hypokalemic PP, Thyrotoxic PP, Hyperkalemic PP, Paramyotonia Congenita von Eulenburg, Hyperkalemic PP with Paramyotonia, the Potassium Aggravated Myotonias and Andersen-Tawil Syndrome.
Hypokalemic Periodic Paralysis
The periodic paralysis are loosely divided into types by how the patient reacts to potassium. In the most common form patients grow weak or paralyzed after foods, medications or events lower the level of potassium in the blood. Strength improves when the patient is given potassium. This form is called Hypokalemic Periodic Paralysis (HypoKPP). Attacks last from hours to days, and range from mild weakness to profound paralysis. Mutations associated with HypoKPP are on the calcium, sodium and potassium channels. Learn More
Thyrotoxic Periodic Paralysis
The second type of HypoKPP is associated with an overactive thyroid gland. This type of HypoKPP is called Thyrotoxic HypoKPP (TPP). It is far more common in Asian males than in females (a ratio of 6 to 1) but is found in people of all races and genders. When physicians say periodic paralysis is only found in Asian males this is the type of periodic paralysis they are thinking of. It isn’t clear how much of a genetic component there is in Thyrotoxic Periodic Paralysis, but a potassium channel gene mutation has been discovered in some patients with TPP. Learn More
Hyperkalemic Periodic Paralysis
Patients with Hyperkalemic PP (HyperKPP) develop paralysis or weakness (and sometimes muscle stiffness) when they eat potassium-rich food. This is also referred to as ‘potassium sensitive’ periodic paralysis. This is usually called Hyperkalemic Periodic Paralysis because most patients’ potassium levels rise during attacks, though not always above normal levels. HyperKPP is due to a mutation in the sodium channel. Learn More
Paramyotonia Congenita
Paramyotonia Congenita (PMC) is a form of periodic paralysis which produces muscle stiffness and weakness in response to cold or exercise. PMC comes in two forms, one in which attacks are always associated with a rise in potassium and a form called Paramyotonia von Eulenburg in which attacks can be associated with hypokalemia. Both result from mutations in the sodium channel. Both can accompany Hyperkalemic Periodic Paralysis or can occur alone. Learn More
Potassium Aggravated Myotonias
The Potassium Aggravated Myotonias (PAMs) are forms of Paramyotonia Congenita in which potassium intake triggers an attack of muscle stiffness. These include Myotonia Fluctuans, which includes short attacks of varying degrees of mild muscle stiffness brought on by exercise, Myotonia Permanens, which causes severe and constant muscle stiffness which is made worse by eating potassium-rich food and exercise, and Acetazolamide-responsive Myotonia Congenita, which causes severe and painfulmuscle stiffness . The muscles appear very well-developed in Acetazolamide-responsive Myotonia Congenita. The PAMs do not cause muscle weakness. Learn More
Andersen-Tawil Syndrome
In Andersen-Tawil Syndrome (ATS) the potassium shifts during attacks of paralysis are inconsistent. Potassium may rise during one attack and fall during another. The traditional classifications of Hypokalemic Periodic Paralysis or Hyperkalemic Periodic Paralysis cannot be applied. Patients also tend to have generalized weakness between attacks. In addition, ATS patients experience irregular heart rhythms including a prolonged QT interval. Some have unusual facial and hand characteristics, such as short stature, clinodactyly (an inward curvature of the 5th fingers), fused or webbed second and third toes, scoliosis (crooked spine), widely spaced eyes, low-set ears, a broad forehead, and a small jaw. These signs may be absent or very subtle, or they may exist in other family members who do not experience muscle weakness or paralysis. Andersen-Tawil Syndrome is inherited in an autosomal dominant pattern. All ATS mutations identified so far have been on the potassium channel. Learn More
reviewed and updated May 2022